
- Home
- News
- Analysis
- States
- Perspective
- Videos
- Education
- Entertainment
- Elections
- World Cup 2023
- Features
- Health
- Budget 2024-25
- Business
- Series
- NEET TANGLE
- Economy Series
- Earth Day
- Kashmir’s Frozen Turbulence
- India@75
- The legend of Ramjanmabhoomi
- Liberalisation@30
- How to tame a dragon
- Celebrating biodiversity
- Farm Matters
- 50 days of solitude
- Bringing Migrants Home
- Budget 2020
- Jharkhand Votes
- The Federal Investigates
- The Federal Impact
- Vanishing Sand
- Gandhi @ 150
- Andhra Today
- Field report
- Operation Gulmarg
- Pandemic @1 Mn in India
- The Federal Year-End
- The Zero Year
- Premium
- Science
- Brand studio
- Home
- NewsNews
- Analysis
- StatesStates
- PerspectivePerspective
- VideosVideos
- Entertainment
- ElectionsElections
- Sports
- Loading...
Sports - Features
- Budget 2024-25
- BusinessBusiness
- Premium
- Loading...
Premium

How the tyranny of digital access is playing out for vaccine seekers
India's vaccine policy has exposed a deep divide in the digital space, wherein, people with digital access, and software developers are able to exploit the CoWIN portal's features to their advantage.

Soon after India opened up registration for COVID vaccination for people aged above 18 years on April 28, Berty Thomas, a 33-year-old Chennai-based investment banker, tried to register on the government’s website for vaccine registration, CoWIN, but he could hardly find any slot. After searching endlessly on the portal, Thomas realised that this was a problem that millions of people across...
Soon after India opened up registration for COVID vaccination for people aged above 18 years on April 28, Berty Thomas, a 33-year-old Chennai-based investment banker, tried to register on the government’s website for vaccine registration, CoWIN, but he could hardly find any slot.
After searching endlessly on the portal, Thomas realised that this was a problem that millions of people across the country were facing, and so, he came up with a solution.
Thomas, who had developed software development as a hobby, leveraged the recently opened up CoWIN Application Programme Interfaces (APIs) to simplify the booking process. He wrote a script in three hours to filter those centres that had slots available for his age group. The next day, he was able to book slots for his wife and himself.
Thomas then posted about it online. Soon, he received a lot of requests from friends and strangers in different cities. Thomas realised the need and soon developed websites above45.in and under45.in and directed users to his Telegram account, where his application automatically fetched real-time data of slot availability on the CoWIN portal and sent alerts to people in the group.
Soon after one got a message, depending on the internet speed and tech access as to how quickly he/she could get on to the CoWIN platform, the users were able to book slots. In most cases, it happened within a minute or two.
In a span of 10 days, his Telegram accounts managed to garner a million followers with 160 groups for different cities across the country.
“I felt happy that I could help so many people. Some thanked me on social platforms, and many wanted to buy a cup of coffee or donate money to manage the server cost or help with whatever ways they can,” Thomas said. He says while he can afford the server cost, he directs those willing to make donations to do it for COVID related fundraisers.
.@_jineshmehta_ at 1 PM: Can we somehow automate logging into CoWIN?
Me: Impossible/Difficult…
10 hours later, I'm running a script that logs me in automatically and tries to reschedule my appointment
— Umang (@umanghome) May 1, 2021
Years ago, Thomas had developed a website unfair.in (now defunct), an airfare prediction application, which told users about the cheapest tickets availability for a particular route they were looking for.
“I’m not a professional programmer. I love programming and I was comfortable writing scripts like this,” he says.
Short-tech-cut to vaccine
But Thomas was not the only one exploiting technology to faster and better way to access vaccines. Many developers across the country came up with similar applications. For instance, the Twitter account @BloreVaccine started sending out updates on Twitter, and the portal Getjab.in sent out updates by mail. Some of these applications refreshed and looked for slots every 5-10 seconds and sent out alters.
While Thomas and the people behind @BloreVaccine were clear that their application did not bypass the CoWIN platform to book slots—they only made the information available to people quickly—some developers tried and wrote scripts to bypass the system and book slots. As a result, many vaccine slots were booked in a matter of seconds automatically, leaving others, sometimes needy people, without vaccine.
Quickly realising the problem, the government cached the appointment availability data by delaying it for 30 minutes and limited the 100 API calls per 5 minutes per IP. Besides it also introduced a 4-digit security code feature before one book the slot.
A techie said this however did not solve the problem and still one could bypass the rules they put in place.
RS Sharma, chairman of the government panel managing the CoWIN platform, reiterated that security measures were in place to tackle the unfair use of the booking vaccine slots even as some challenged him on Twitter.
https://twitter.com/pranavkojha/status/1393399410541817858
However, there seemed to be another problem due to the highly acclaimed CoWIN portal that those with internet access could exploit. Many in the cities, who were unable to find vaccine slots nearby, chose to get their jabs in neighbouring villages districts.
Much on the lines of people going to neighbouring districts in search of intensive care units and oxygenated beds due to shortage in Bengaluru, the dearth of vaccines pushed some to go to Mysuru, about 150 km from the state capital to get the vaccines.
This drew the ire of the locals who accessed the vaccine by just walking in to the centre. On the other hand, those who booked slots online questioned why those who didn’t have bookings were being given vaccines.
Moreover, as private players like Apollo and Manipal offered vaccines at prices ranging from ₹850 to ₹1,350 per dose, many couldn’t afford them.
My colleague did the same (Ramanagara), was asked to turn around or get his car impounded. Strict ‘No’, speak in Kannada, explain the situation. The police were actually irate on him not waiting for vaccine in his ward, that feeling is mutual with me too .
— Christo (@christodharry) May 10, 2021
Need for checks and balances
Osama Manzar, director of the non-profit Digital Empowerment Foundation in Delhi, says that at least 80 crore or 60% of the country’s population do not have access to internet, money or English-language abilities, which are key to getting the vaccine.
“If technology can make my life better, it’s appreciable. But we must remember that the technology is not available to all in India,” Manzar said. “It’s only favouring the rich as not many are able to walk in and get the slots.”
Manzar feels the vaccination drive is exclusionary. His team is looking to file a public interest litigation to challenge this digital divide and make the portal accessible in regional languages.
To such criticisms, Thomas says his only goal is to help people and if that benefits only a section of society, it is not he who created these barriers.
“The checks and balances should be put in place by the government and fixed at the policy making level,” he says. “With the available APIs, I only democratised the information availability. One cannot blame us for that.”
Thomas is in fact even willing to collaborate with governments and help district administrations if they wish to cater to people in their region. “We have also been encouraging people who use our service to also help those who are deprived of technology,” he says.
Another developer, a 20-year-old student collaborating with Thomas, who wished to remain anonymous, says the system is faulty and not right. “But the government should be held accountable for it.”
“Some of us are thinking of approaching the government and asking them to change a few things or take our help in improving the system,” he says.
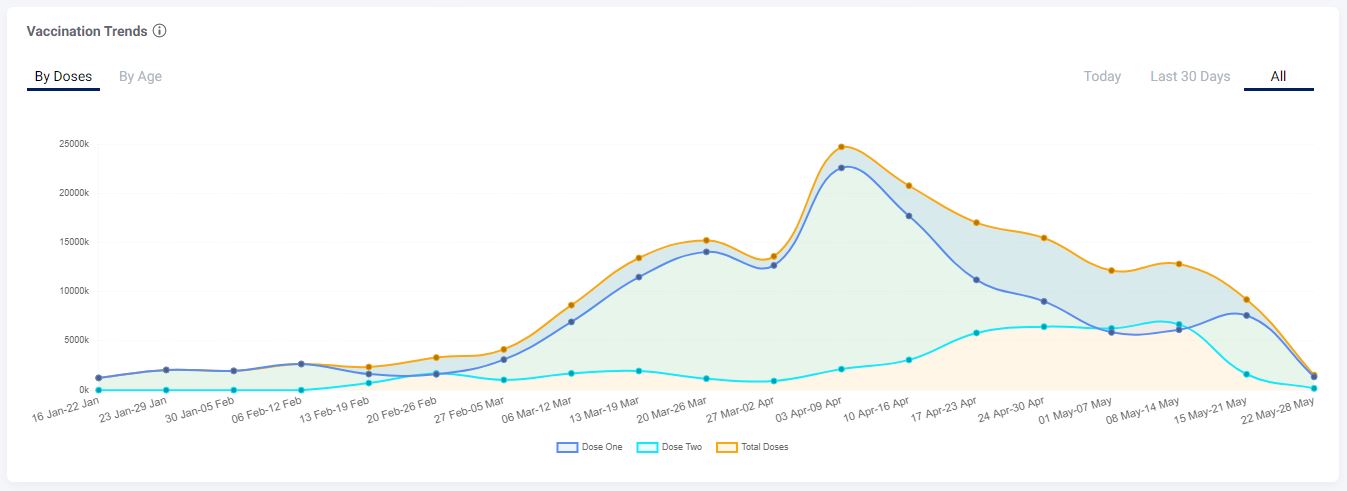
The vaccination drive started in India on January 16. Five months down the line, the country has managed to vaccinate less than 15% of the population. As of May 20, India’s cumulative vaccination coverage stood at 18.70 crore dosages (1st Dose: 14.46 crores and 2nd Dose: 4.23 crore).
and Sharma even said India was ready to share its experience and expertise on CoWIN to other countries.
Speaking at a webinar organised by the New Delhi-based think tank Research and Information System for Developing Countries (RIS), Sharma said India’s “rich experience” of vaccinating people and the challenges it faced amid the linguistic and demographic barriers, could be shared with other countries, especially from the developing world. He added that Nigeria has requested India to share the details.
Sylvia Karpagam, a public health expert in Bengaluru, was of the view that the vaccine policy and CoWIN registration and booking requirement was an elitist way of looking at things.
She says that some people in semi-urban or rural areas find it difficult to even handle a gadget and struggle to send images of doctor’s prescriptions.
While developers cannot be blamed, she says technology can aid a good health system, but in the absence of it, it only turns abusive and excludes the most vulnerable sections of the society, alienating them further from healthcare facilities.
“I feel the government did it deliberately as they had no mechanism in place. There’s not even a grievance redressal system in place,” she says. “It’s completely non-transparent and lacks accountability.”
