India’s discharge policy behind increased COVID recovery rate: Experts
India crossed the 3 lakh-mark as it reported the highest single-day spike of 11,458 new COVID-19 cases on Saturday.

India crossed the 3 lakh-mark as it reported the highest single-day spike of 11,458 new COVID-19 cases on Saturday (June 13).
According to the Ministry of Health, the total cases rose to 3,08,993, of which 1,45,779 are active cases while 1,54,330 were cured/discharged/had migrated, and with 386 deaths registered in the last 24 hours, the death toll rose to 8,884 in the country.
But according to the health ministry, the recovery rate is increasing rapidly since it is reportedly surpassing the number of active cases in the country. According to the health ministry, the recovery rate in the country has improved to 48.19 per cent in May when compared to a mere 11.42 per cent in April. In June, the recovery rate went up to nearly 50 per cent.
On May 26, Lav Agarwal, Joint Secretary of the Union health ministry, said the recovery rate in India has been increasing, since it was 7.1 per cent in March, 11.42 per cent in April, 26 per cent in the beginning of May, and 41.61 per cent now.
However, health experts claim that the recovery rate is improving because of the government’s revised discharge policy.
The guidelines, which were revised on May 8, state that there is no need for testing for mild and moderate cases of COVID-19 before they are discharged, and that only severe cases of COVID-19 will be tested before discharge.
Dr K R Anthony, a consultant on public health, child survival and development in Kochi, said this was a “very normal thing” and that with time, the recoveries would also increase.
However, the changed criteria for early discharge appeared to boost the recovery numbers artificially.
Earlier, all patients were tested and discharged only when their chest radiograph exam was cleared and two consecutive RT-PCR tests (conducted for COVID-19) returned negative.
According to the new guidelines, patients can be discharged after 10 days of symptom onset and no fever for three days for mild/very mild/pre-symptomatic cases. There is no need for testing prior to discharge, and the patient will be advised to remain isolated at home and self-monitor his/her health for seven days.
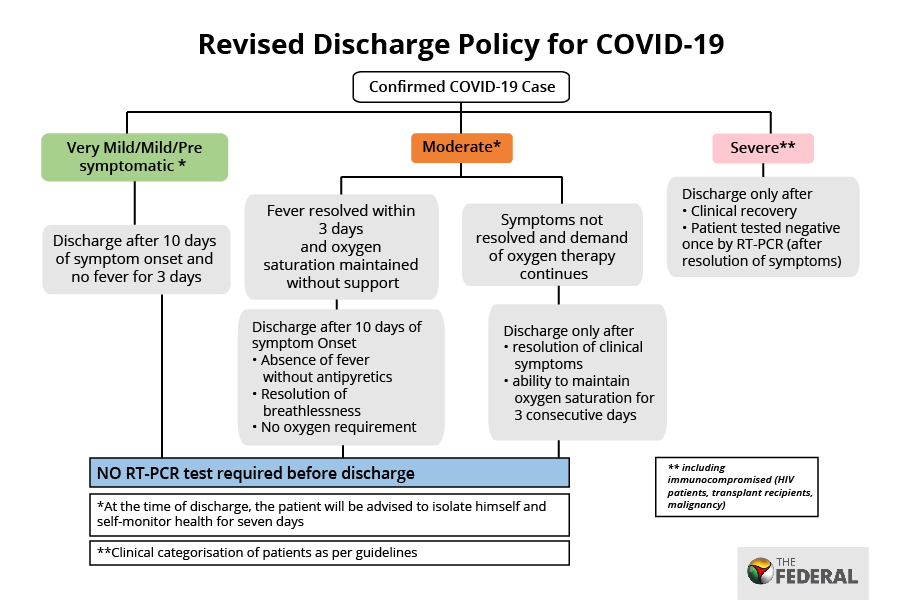
For moderate cases, patients can be discharged if they are asymptomatic for three days or after 10 days of symptom onset. Similar to the mild cases, there is no need for testing prior to discharge and the patient will be advised to remain isolated at home and self-monitor his/her health for 7 days.
However, for severe cases, the patient will be discharged only after clinical recovery and if the patient tests negative once in the RT-PCR test after the symptoms subside.
Dr K K Aggarwal, President of the Heart Care Foundation of India, said 70 per cent of people do not show any major symptoms and that discharging before proper testing can increase the number of positive cases, since the patient might think he was cured when he was not, and infect many others while coming in contact with them.
However, the health ministry also claimed the available evidence does not indicate any increase in the risk of virus transmission from patients discharged since they would have been advised to stay in isolation for seven days.
They further said several countries have changed the criteria for discharge from ‘test-based strategy’ to ‘symptom-based strategy’ or ‘time based strategy’.
A review of ICMR’s laboratory surveillance data also indicated that after the initial RT-PCR positive results, patients tested negative for the coronavirus after a median duration of 10 days.
Recent studies have also suggested that the viral load peaks in the pre-symptomatic period (two days before symptoms appear) and subsides over the next seven days, the health ministry added.
Concern over COVID-19 death rate
Dr K Srinath Reddy, President, Public Health Foundation of India questioned, “The number of deaths due to COVID-19 is increasing every day. How can we say that the number of recoveries is coming down?”
He also said, “Until the time the number of deaths fall, we cannot say the recovery rate is increasing and, actually, the death rate should be watched now, not cases.”
The sharp contrast in death rates can be seen in the fact that 132 people died due to COVID-19 on May 13, and 386 people died a month later on June 13.
The death toll on June 13 happens to be the highest single-day tally due to COVID-19 in India.
The total number of deaths has increased from 2,551 till May 13, 2020 to 8,884 till June 13, 2020. No deaths due to COVID-19 were recorded in India until February.
In March, 35 people died, while 1,119 fatalities were reported in April. The month of May saw 4,254 deaths, while the first 13 days of June witnessed 3,476 deaths.
Despite the spike in numbers, the health department has been saying that the case fatality rate (CFR) in India is one of the lowest in the world, and that the fatality rate, which was 3.3 per cent a month ago, has been reduced to 2.8 per cent. India’s fatality rate is ranked 25th in the world, with Italy and the United States at the top.
However, the death rate due to COVID-19 is not conclusive or accurate since a person who dies before being brought to the hospital is not tested.
The expert believes that the death rate is not calculated properly in India and if it is calculated properly, it would have been approximately 5.5 per cent now.
Dr Anthony said the government’s calculation of the recovery rate masks the increase in active cases whose outcome is not known yet.
He further said that before the stoppage of a daily media briefing by the joint secretary of the Ministry of Health and Family Welfare (MoHFW), there was a problem in understanding the figures stated by the Health Ministry on death rate and recovery rate.
“The problem was quoting a moving cumulative total positive cases as the denominator and the numerator being deaths or recovered cases. The actual denominator should have been the total number of closed cases where the outcome is crystal clear, either death or recovery,” Dr Anthony said.
As an example, Dr Anthony noted the number of recovered cases down and added that to the deaths reported on the briefing day to obtain the denominator, which is the overall outcome.
“Accordingly, 5.46 per cent is the CFR. Where did the ministry’s technical advisors get this figure of 2.8 per cent CFR, I fail to understand,” Dr Anthony pointed out.